In the past several days, through the lens of my profession, I have been given a rather stark and disturbing vision of our current cultural revolution. It is, it seems, a revolution every bit as pervasive and transformational — and destructive — as China’s Cultural Revolution of the 60s — and indeed may be but a different manifestation of a global transformation which transpired in those very same decades in the West. Ideas have consequences, as they say, and we are watching them bear fruit before our very eyes in a slow-motion train wreck which seems now to be accelerating at a disturbing rate.
In the past several days, through the lens of my profession, I have been given a rather stark and disturbing vision of our current cultural revolution. It is, it seems, a revolution every bit as pervasive and transformational — and destructive — as China’s Cultural Revolution of the 60s — and indeed may be but a different manifestation of a global transformation which transpired in those very same decades in the West. Ideas have consequences, as they say, and we are watching them bear fruit before our very eyes in a slow-motion train wreck which seems now to be accelerating at a disturbing rate.
Exhibit 1: Phyllis Chesler’s recent piece, “Every hospital patient has a story”, at PajamasMedia. It is a piece to be read to completion, including its lengthy comment section. Therein she details a recent experience during a hospital stay for a hip replacement, with a rather remarkable litany of rudeness, neglect, indifference, and suffering sustained at the hands of her healers, at an upscale New York hospital. Her story is shocking enough, and revelatory; the comments provide even further insight, running the expected gamut of such a piece in the New Media. There are those simply shocked; those sharing similar horror stories; those relaying far better experiences in contrast; those defending doctors and nurses, those attacking them. There is the obligate wackjob who blames the AMA, and the usual finger-pointing: not enough nurses, too much paperwork, inadequate pay scales to draw quality; the evil insurance companies and the government. All mostly true, to greater or lesser degree — but all missing the core dysfunction by a wide mark. At the final period of her post, one comes away with a sense of hopeless, feeling out of control and angry, despairing that such a situation may be even a part of our reality (and not knowing how large a part it may be), yet at a loss to prevent its malignant progression through our remaining hospitals which may have been spared to date, the encroachment of such a toxic stew of callousness, indifference, and coldness. There seems, in the end, little cause for optimism.
Exhibit 2: It is late, nearly 9 P.M., seeing a final consult at the end of a punishing call day, in the ICU. The patient, chronologically young yet physiologically Methuselan, lies in his bed, oxygen mask affixed to his face by heavy straps, bleeding, as he has for months, from a tumor in his kidney. He would not survive surgery, nor even radiological intervention to stem the hemorrhage by strangling its arterial lifeline. He is, furthermore, in the parlance of modern medicine, “non-compliant”: refusing treatments and diagnostic studies; rude and abusive to nurses and physicians alike; demanding to go home though unlikely to survive there for any significant length of time.
The nurse — young, competent, smart, hard-working, the very best of the modern nursing profession — apprises me of his situation, closing with this knockout punch: “You know, we just passed that initiative — you know, the suicide one. He’d be an excellent candidate.”
She wasn’t joking.
Taken a bit off guard, I responded that it is most unwise to give physicians the power to kill you, for we will become very good at it, and impossible to stop once we are.
She continued: “No, I would love to work for a Dr. Kevorkian. Be an Angel of Death, you know?”
“I know”, I muttered under my breath, as she ran off to another bedside, competently and with great efficiency, to adjust some ventilator or fine-tune some dopamine drip. And hopefully do nothing more.
These vignettes in modern medicine are really not about medicine at all. They are in truth about a culture which has lost its compassion. Our calloused and cynical society has become a raging river fed by a thousand foul and fetid streams. We have, by turns, taught our children that ethics are situational and values neutral; taught our women that compassion and service are signs of weakness, that they must become hard and heartless like the men they hate; taught our men that success and the respect of others comes not through character and integrity but through callousness, cynicism, and greed; and taught ourselves that we are a law unto ourselves, the sole and final arbiter of what is right and what is good.
We have, in our post-modern and post-Christian culture, inexorably and irrevocably turned from our roots in Christian morality and worldview, which was the foundation and font of that which we now know — or used to know — as Western Civilization. Yes, we have preserved the tinsel and the trappings, the gilded and glittering exterior of a decaying sarcophagus, where we speak self-righteously of rights while denying their origin in the divine spark within the human spirit, made in the image of God; where we bray about liberty, but are enslaved to its bejeweled impostor, the damsel of decadence and libertinism; where compassion is naught but another government program to address the consequences of our own aberrant and irresponsible behavior, duly justified, rationalized, and denied. Others must pay so that I may play, you know.
This toxic stew of self-centered callousness has percolated into every pore of our society. In health care, the effects are universal and pernicious. Patients demand perfection, trusting the wisdom of a web browser over the experience of a physician — then running to their attorney to redress every poor outcome which their disease or their destructive lifestyles have helped bring about. Physicians, hardened and cynical from countless battles with corrupt insurance companies, lawyers, and Stalinist government regulation, forget that they exist solely to serve the patient with compassion and self-sacrifice, and that financial recompense is secondary to healing and empathy. Nurses have in large measure become administrators, made ever more remote from their patients by mountains of paperwork and impossible nurse-to-patient ratios, their patient-critical tasks delegated to underlings poorly trained and ill-treated. Hospital administrators are MBAs, with no interest or clue about what constitutes good health care, and are indifferent so long as their departments are profitable and their marketing wizards successful as they trumpet “Care with Compassion” in TV ads, radio, and muzac on hold.
The list could go on far longer, but the theme is clear: we have as a culture become utterly self-focused, trusting no one, demanding our rights while neglecting our responsibilities, seeking to be profitable rather than professional. We have abandoned the responsibility to be patient and caring of others, forgiving of human shortcomings and humble about the limits of our abilities — a responsibility not merely of those in health care but of human beings in civil society. We have, through the dubious gift of extraordinary technological advances, industrialized our profession, and replaced a sacred covenant of commitment to the patient’s best — and its corollary of the patient’s trust in the integrity and motives of physicians and nurses — with the cold legality of contract medicine. Small wonder we are treated as fungible commodities in doctors’ offices and hospital beds. Small wonder we will be euthanized when we have exhausted our compassion quotient, dispatched by highly efficient providers delivering “Death with Dignity.”
This utter self-obsession and cynical callousness is by no means limited to health care. We long for “bipartisanship” in government (by which we hope for reasoned men of principle to come together for the good of those they represent), but get instead the blood-lust of modern politics, where power trumps principle, money is king, and votes are bought and sold like chattel. Lawyers sue everything that breathes — and much that doesn’t — raking in billions while their “victimized clients” get pocket change they can believe in. Airlines pack in passengers like cattle, lose your bags, and toss you a bag of peanuts for your trouble. Road rage is rampant, rudeness rules, rip-offs too common to count. The coarseness in culture is extraordinary — in language, art, media, fashion, and behavior. It is revealing how shocked we find ourselves when encounter someone — regardless of the venue — who is actually pleasant, helpful, courteous, and kind; we have come to expect and tolerate far worse as a matter of course.
The revolution which started in the 60s with the “me” generation is bearing its bitter fruit — though its aging proponents will never admit it. And sadly, there’s no going back: the changes which have infiltrated and infected the culture, inoculated through education, media, entertainment, scientific rationalism, and a relentless and highly successful assault on reason and tradition, are permanent, and their consequences will only grow in magnitude.
So it’s time for a counter-revolution.
There is an alternative to our current cultural narcissism with its corrosive, calloused, destructive bent. It is not a new government program, nor a political movement; no demonstrations in the street, no marches on Washington. Its core ideology is over 2000 years old, and the foot soldiers of the revolution are already widely dispersed throughout the culture.
This revolutionary force is called Christianity, and it’s long past time to raise the banner and spring into action.
The true antidote to the nihilism and corruption of the age will be found, as it has always been, in the church. It has since its inception been a revolutionary force, transforming the hopeless and purposeless anarchy of the pagan world of its infancy by bringing light, hope and joy where there was none before.
It can happen again.
The church, of course, has to no small degree been co-opted by the culture it should have transformed. From TV evangelists preaching God-ordained health and wealth to liberal denominations rejecting the core truths of their foundation and worshiping instead the god of government and humanistic socialism; from pederast priests to episcopal sodomy, Christianity in the West has whored itself to a prosperous but decadent culture. Its salt has lost its saltiness, and it has, not surprisingly, been trampled underfoot by men.
It is time to return to our First Love. It is time once again to become light to an dark and stygian world. It is time for a revolution of the soul.
We must, first and foremost, be about grace and truth. We must begin with the truth of our calling: to be holy, transformed by the power of Christ and the work of the Spirit. We are, by nature of our new birth in Christ, His ambassadors: we are to be the face, the hands, the heart, the words, the compassion of Him who saved us.
The task is enormous, yet for each of us, the steps are small, easily achievable yet enormously powerful.
It must begin with a renewed commitment to obedience and submission to Christ, a willingness to fully subject ourselves to His will, rather than trying to bend His will to ours. It means getting serious about church attendance — not merely as a consumer but as an active participant. We need to renew our devotion to prayer, to Scripture reading, study, and memorization, to fellowship with other Christians. These are simple steps which ground us in truth, and give us access to that power which can first of all transform us, then radiate out to all around us.
Then we must act like the counter-culturists we claim to be. Be patient with those who are difficult; be generous in time and money; express gratitude to those around us (when was the last time you wrote a thank you note to your doctor, your contractor, your attorney, to the manager of the store employee who helped you?). Lose the profanity; guard your tongue. Repair broken relationships, as best you can. Be joyful in difficult times, knowing that God is at work in your life despite your difficulties. Be compassionate rather than judgmental to those whose life choices are destructive or misguided. The tattoos and piercings we ridicule are cries of desperation from those hungering for purpose and meaning.
These things will not come easily to many of us who claim to be Christians, as we have become complacent in our self-gratification and comfortable compromises, fearful of being viewed as extremist or weird, rejected and ridiculed.
Get over it.
You may just find that such renewed passion for Christ and love for others might, just might, transform your life.
And you might just find that it will change the world.
Got a better idea? Good, I didn’t think so.
Let’s get started.
 Over at Big Government, we get a glimpse of where ObamaCare will take us: Health Care’s Coming Heart Attack – A Pre-Obama Care Death Panel?
Over at Big Government, we get a glimpse of where ObamaCare will take us: Health Care’s Coming Heart Attack – A Pre-Obama Care Death Panel?


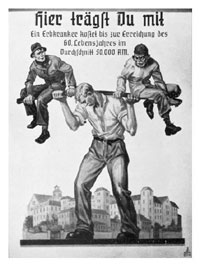 In the years following the Great War, a sense of doom and panic settled over Germany. Long concerned about a declining birth rate, the country faced the loss of 2 million of its fine young men in the war, the crushing burden of an economy devastated by war and the Great Depression, further compounded by the economic body blow of reparations and the loss of the German colonies imposed by the Treaty of Versailles. Many worried that the Nordic race itself was threatened with extinction.
In the years following the Great War, a sense of doom and panic settled over Germany. Long concerned about a declining birth rate, the country faced the loss of 2 million of its fine young men in the war, the crushing burden of an economy devastated by war and the Great Depression, further compounded by the economic body blow of reparations and the loss of the German colonies imposed by the Treaty of Versailles. Many worried that the Nordic race itself was threatened with extinction. I hope to have more to say on the issue of euthanasia and assisted suicide in the near future. In the meantime, I highly recommend
I hope to have more to say on the issue of euthanasia and assisted suicide in the near future. In the meantime, I highly recommend